Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis

1
Department of Epidemiology, German Institute of Human Nutrition Potsdam-Rehbruecke (DIfE), Arthur-Scheunert-Allee 114-116, 14558 Nuthetal, Germany
2
Department of Molecular Epidemiology, German Institute of Human Nutrition Potsdam-Rehbruecke, 14558 Nuthetal, Germany
3
Department of Nutritional Sciences, University of Vienna, Althanstraße 14, 1090 Vienna, Austria
*
Author to whom correspondence should be addressed.
Nutrients 2017, 9(10), 1063; https://doi.org/10.3390/nu9101063
Submission received: 16 August 2017
/
Revised: 5 September 2017
/
Accepted: 21 September 2017
/
Published: 26 September 2017
(This article belongs to the Special Issue Assessing the Mediterranean Diet in Public Health: Scoring Systems, Effects on Chronic Disease and Interventions)
Abstract
:The aim of the present systematic review and meta-analysis was to gain further insight into the effects of adherence to Mediterranean Diet (MedD) on risk of overall cancer mortality, risk of different types of cancer, and cancer mortality and recurrence risk in cancer survivors. Literature search was performed using the electronic databases PubMed, and Scopus until 25 August 2017. We included randomized trials (RCTs), cohort (for specific tumors only incidence cases were used) studies, and case-control studies. Study-specific risk ratios, hazard ratios, and odds ratios (RR/HR/OR) were pooled using a random effects model. Observational studies (cohort and case-control studies), and intervention trials were meta-analyzed separately. The updated review process showed 27 studies that were not included in the previous meta-analysis (total number of studies evaluated: 83 studies). An overall population of 2,130,753 subjects was included in the present update. The highest adherence score to a MedD was inversely associated with a lower risk of cancer mortality (RRcohort: 0.86, 95% CI 0.81 to 0.91, I2 = 82%; n = 14 studies), colorectal cancer (RRobservational: 0.82, 95% CI 0.75 to 0.88, I2 = 73%; n = 11 studies), breast cancer (RRRCT: 0.43, 95% CI 0.21 to 0.88, n = 1 study) (RRobservational: 0.92, 95% CI 0.87 to 0.96, I2 = 22%, n = 16 studies), gastric cancer (RRobservational: 0.72, 95% CI 0.60 to 0.86, I2 = 55%; n = 4 studies), liver cancer (RRobservational: 0.58, 95% CI 0.46 to 0.73, I2 = 0%; n = 2 studies), head and neck cancer (RRobservational: 0.49, 95% CI 0.37 to 0.66, I2 = 87%; n = 7 studies), and prostate cancer (RRobservational: 0.96, 95% CI 0.92 to 1.00, I2 = 0%; n = 6 studies). Among cancer survivors, the association between the adherence to the highest MedD category and risk of cancer mortality, and cancer recurrence was not statistically significant. Pooled analyses of individual components of the MedD revealed that the protective effects appear to be most attributable to fruits, vegetables, and whole grains. The updated meta-analysis confirms an important inverse association between adherence to a MedD and cancer mortality and risk of several cancer types, especially colorectal cancer. These observed beneficial effects are mainly driven by higher intakes of fruits, vegetables, and whole grains. Moreover, we were able to report for the first time a small decrease in breast cancer risk (6%) by pooling seven cohort studies.
1. Introduction
Mortality rate due to cancer has been decreasing since the 1990s, most likely due to improved measures of preventive examinations as well as therapeutic interventions. However, this heterogeneous complex of diseases still remains one of the major causes of premature death worldwide as it is ranked second to cardiovascular diseases in current statistics [1]. Cancer incidence is estimated to be 18% by the year 2030 [2].
Tumors are regarded to be an age-dependent phenomenon. Despite this, cancer and other chronic diseases increasingly manifest themselves at a younger age [3]. This emphasizes the fact that the growing incidence of malignant diseases is not exclusively attributable to an increase in life expectancy, but rather due to a number of basic environmental and lifestyle risk factors. Approximately 5–10% of all tumor diseases are caused by genetic predisposition, while the pathogenesis of the remaining 90–95% can be explained by unfavorable environmental conditions or an unhealthy lifestyle [4]. The latter can mainly be characterized by an unbalanced diet, lack of exercise, and consumption of alcohol and tobacco [5].
These are modifiable risk factors, meaning that the manifestation of many types of cancer can be prevented or at least postponed. The World Cancer Research Fund (WCRF) assumes that 3–4 million cases of cancer worldwide might be avoided by adopting a healthier lifestyle [6]. The transition from a detrimental to a beneficial lifestyle cannot always be reduced to a simple formula, e.g., abstention in the case of tobacco consumption. It has been suggested that approximately 30% of cancers can be prevented by a healthy diet [7], however, foods simultaneously contain both ingredients that are protective and others that may cause harm. Some specific bioactive compounds from foods with tumor-preventive potential have been characterized in the past, e.g., polyphenols, n-3 fatty acids, or monounsaturated fatty acids [8]. By contrast, alcohol or nitrosamines were identified as ingredients correlated with an increased risk of cancer [9,10,11]. Another very important aspect in this regard is the growing number of cancer survivors. Since its first mention by Fitzhugh Mullan in 1985 [12], this term has not been given a distinct definition. However, it is generally acknowledged to include patients with diagnosed cancer who have carried out all required therapeutic measures and are currently showing no symptoms of disease (in remission). This group of the population still has to cope with side-effects of their specific therapy as well as the threat of recurrence. Due to heightened awareness of the necessity of check-ups and routine examinations as well as evolved diagnostic and therapeutic tools, it is reasonable to speculate that the number of cancer survivors will increase substantially in the years ahead [13,14,15].
Dietary interventions will represent an effective measure in secondary/tertiary prevention or as a part of an adjunctive therapy. Despite this, there are at present very few evidence-based nutritional recommendations for cancer survivors [6,16].
Rather than focusing on single nutrients, the assessment of dietary patterns might be a more adequate approach to clarify the connections between nutrition and cancer. In contrast to associations based on single-nutrient analyses, dietary patterns allow for a simultaneous assessment of favorable and unfavorable components in food as well as their interdependencies [17,18]. The Mediterranean diet (MedD) belongs to the a priori defined dietary patterns. For this type of pattern, adherence to a regimen settled in advance has been extensively assessed and consecutively associated with health parameters [19]. The term MedD was coined by Keys and co-workers after observing significantly lower rates of coronary heart disease in countries bordering the Mediterranean Sea (Cyprus, Greece, and Italy) as compared to The Netherlands, USA, or Finland [20,21].
A MedD is characterized by a high consumption of plant-based foods, especially whole grain products, vegetables, fruits, nuts, and legumes with regular intake of fish and seafood. Eggs, red and processed meat as well as high-fat dairy products are consumed in low amounts [19,22,23]. Additional indicators often used to describe a MedD are moderate alcohol consumption, preferably red wine taken with meals. Fat is predominately provided in the form of olive oil [24,25,26]. Taken together, this results in a dietary pattern with a low content of saturated fatty acids (7–8% of daily total energy consumption) and a total percentage of fat of 30–40% per day [27].
Despite the limitations regarding the exact recording of the adherence to a MedD and the small number of studies investigating corresponding pathogenetic mechanisms, systematic reviews and meta-analyses of observational studies provide evidence that a MedD exerts protective functions with respect to tumor incidence and mortality [28,29,30,31]. In a clinical trial, choice of diet orientated towards a Mediterranean pattern was found to be associated with reduced all-cause mortality as well as a 61%-decrease in cancer incidence [32]. In addition, a primary-preventive effect of a MedD supplemented with extra-virgin olive oil on breast cancer was reported [33].
We decided to update our previous meta-analyses on the topic of MedD and cancer [28] for the second time due to the following reasons: a number of additional epidemiological studies and randomized controlled trials (RCTs) investigating the correlations between MedD and risk of cancer have meanwhile been published and will therefore allow for a more comprehensive synthesis of the corresponding data; the same applies for studies investigating the effects of MedD in cancer survivors (where the previous analysis did not yield any significant correlation between adherence to MedD and cancer mortality or recurrence); new types of cancer localizations have been taken into consideration. In addition, to gain further insights into the complex relationship between diet and cancer, we analyzed the effects of specific food groups typical of the MedD on tumor incidences in this update.
2. Methods
The review protocol of the previous versions of the systematic review is registered in PROSPERO International Prospective Register of Systematic Reviews (https://www.crd.york.ac.uk/prospero/display_record.asp?ID=CRD42013004382).
2.1. Data Sources and Searches
A literature search was performed using the electronic databases PubMed (25 August 2017), and Scopus (25 August 2017) using the following search terms for PubMed (Appendix A).
The search strategy had no language restrictions. Moreover, reference lists from reviews, meta-analyses, and the retrieved articles were searched to identify further relevant studies. Literature search was conducted by one author (LS), with questions or uncertainties resolved by discussion with another author (GH).
2.2. Study Selection
Cohort studies and case-control studies investigating the association between the MedD and risk of cancer mortality and cancer types in the general population; cancer mortality and cancer recurrence among cancer survivors were included in this update [29].
2.3. Data Extraction
The following data were extracted from each study as reported in the previous version [29]: name of first author, country, study name, study design, outcome, population size, follow-up, age at entry, sex, components of score, score range, adjustment factors, and risk estimates (most adjusted Hazard ratio (HR), Risk ratio (RR) or Odds ratio (OR) comparing highest vs. lowest adherence category) with their corresponding 95% CIs.
2.4. Definition: Adherence to Mediterranean Diet
The two intervention trials differed regarding food components in the MedD intervention groups. Whereas higher intakes of plant based foods such as vegetables, fruits, nuts and legumes were recommended in the PREDIMED as well as the Lyon Diet Heart study, the recommended fat source in the PREDIMED study was extra virgin olive oil and nuts, whereas in the intervention group in the Lyon Heart Study was supplemented with rapeseed oil margarine [34,35].
For observational studies meta-analysis, the lowest adherence to MedD category was compared with the highest MedD category (according to the MedD scores by Trichopoulou [36], Fung [37], or Panagiotakos [38]; with the exception of six studies that used factor analysis or principal component analysis to define the MedD (authors named these MedD pattern): Menotti et al. (2011) [39] (HR: per 1 standard deviation increase), Murtaugh et al. (2008) [40] (OR: fourth vs. first quartile), Cottet et al. (2005) [41] (OR: third vs. first tertile), Bessaoud et al. (2012) [42] (OR per increment of one standard error), Castello et al. (2017a) [43] (OR: fourth vs. first quartile), and Castello et al. (2017b) [44] (OR: fourth vs. first quartile). The maximum ranges of the different MedD scores are reported in Table 1.
2.5. Statistical Analysis
The meta-analysis was performed by combining the multivariable adjusted RRs, HR or ORs of the highest compared with the lowest MedD adherence category based on random effects model using the DerSimonian-Laird method, which incorporated both within and between study variability [45]. Because outcomes were not very rare and heterogeneity modeling was deemed important, the random effects model was used.
A second meta-analysis was performed to compare the effects of the different dietary components of the Mediterranean dietary pattern on overall cancer risk, based on data given within the papers included in the present meta-analysis. To evaluate the weighting of each study, the standard error for the logarithm HR/RR/OR of each study was calculated and regarded as the estimated variance of the logarithm HR/RR/OR, using an inverse variance method [45]. For the high vs. low adherence to MedD adherence category studies were grouped according to the different clinical outcomes (overall risk of cancer mortality, and risk of colorectal cancer/breast cancer/prostate cancer/gastric cancer/head and neck cancer/esophageal cancer/pancreatic cancer/liver cancer/ovarian cancer/endometrial cancer/respiratory cancer/bladder cancer/gallbladder cancer/biliary tract cancer/and lymphoma). Observational studies (cohort and case-control studies), and intervention trials were meta-analyzed separately. Meta-analysis was stratified for observational studies by study design: cohort studies, and case-control studies.
Heterogeneity was estimated by the Cochrane Q test together with the I2 statistic. An I2 value >50% indicates substantial heterogeneity across studies [46,47]. Potential small-study effects, such as publication bias, were explored using Egger’s test and funnel plots when at least 10 studies were available, as recommended by the Cochrane Handbook [48]. All analyses were conducted using the Review Manager by the Cochrane Collaboration (version 5.3 Copenhagen: The Nordic Cochrane Centre) and Stata 12.0 (Stata-Corp, College Station, TX, USA).
3. Results
3.1. Literature Search and Study Characteristics
The detailed steps of the updated meta-analysis article search (Supplementary Materials Figure S1) and selection process are given as an adapted Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram [49].
Taken together, 83 studies [32,33,37,39,40,42,43,44,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124] were included in the present systematic review update (27 additional studies (two randomized trials [32,33], 16 cohort studies [50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65], and nine case-control studies [43,44,66,67,68,69,70,71,72]) were identified that were not included in the previous meta-analyses [28,29]).
General characteristics of these additional studies are summarized in Table 1. For the present updated meta-analyses, data of new studies were synthesized together with the data of the previous reports. Overall, two RCTs, including 4887 subjects; 51 cohort studies including 2,025,303 subjects (incidence cases; biliary tract: 163; bladder: 1804; breast: 18,782; colorectal: 15,108; endometrial: 1392; esophageal: 848; gallbladder: 77; gastric: 1382; head and neck: 1868; liver: 509; pancreatic: 865; prostate: 29,806; ovarian: 696; respiratory: 9875); and 30 case-control studies with 100,563 subjects met the objectives and were included in the updated meta-analysis. An overall population of 2,130,753 subjects was included in the present update.
3.2. Main Outcomes
Documentations of the different clinical outcomes are distributed as follows: overall risk of cancer mortality was evaluated in 14 cohorts and one RCT; breast cancer risk in one RCT, seven cohorts and nine case-control studies; colorectal cancer risk in six cohorts and five case control studies; prostate cancer risk in three cohorts and three case-control studies; gastric cancer risk in two cohorts and two case-control study; head and neck cancer in one RCT, in one cohort study and six case-control studies; endometrial cancer in one cohort and two case-control studies; respiratory cancer in one RCT, and three cohort studies; bladder cancer in two cohort studies; liver cancer, pancreatic cancer and esophageal cancer in one cohort study and one case-control study; ovarian, gallbladder, and biliary tract cancer in one cohort study each; lymphoma in one case control study; cancer mortality among cancer survivors in four cohort studies; cancer recurrence among cancer survivors in one cohort study; and cancer-specific mortality in one cohort study.
Using a random effects model, we found that the highest adherence score to the MedD was inversely associated with a lower risk of overall cancer mortality (RRcohort: 0.86, 95% confidence interval (CI) 0.81 to 0.91; I2 = 81%; n = 15 studies) but not among one RCT (RRRCT: 0.75, 95% CI 0.17 to 3.33, I2 = NA) (Supplementary Materials Figure S2, Table S2). Among cancer survivors, we observed no association between the adherence to the highest MedD category and risk of cancer mortality (RR: 0.95, 95% CI 0.82 to 1.12; I2 = 5%; n = 4 studies) (Supplementary Materials Figure S3). Moreover, high adherence to a Mediterranean dietary pattern was inversely associated with risk of colorectal cancer (RRobservational: 0.82, 95% CI 0.75 to 0.88; I2 = 73%, n = 11 studies; RRcohort: 0.86, 95% CI 0.80 to 0.92, I2 = 28%, n = 6 studies; RRcase-control: 0.71, 95% CI 0.57 to 0.88, I2 = 88%, n = 5 studies) (Supplementary Materials Figure S4) and breast cancer (RRRCT: 0.43, 95% CI 0.21 to 0.88, I2 = NA%, n = 1 study; RRobservational: 0.92, 95% CI 0.89 to 0.96, I2 = 8%, n = 16 studies; RRcohort: 0.94, 95% CI 0.90 to 0.99, I2 = 11%, n = 7 studies; RRcase-control: 0.89, 95% CI 0.85 to 0.94, I2 = 0%, n = 9 studies) (Supplementary Materials Figure S5). With respect to incidence of all other different types of cancer, results are summarized in Table 2 and the corresponding forest plots are given in Figures S2–S20.
3.3. Food Group Components of the MedD and Risk of Cancer
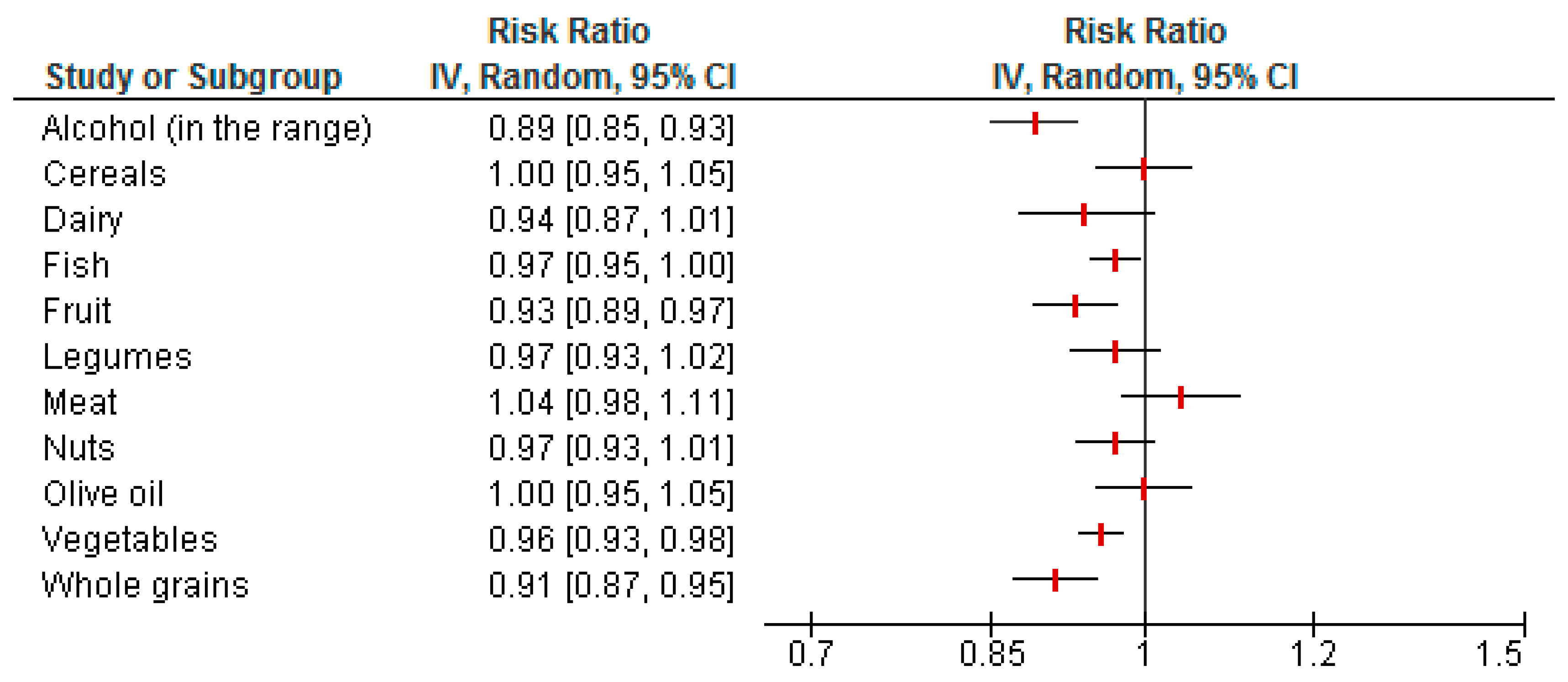
Pooled estimates for the single components of the Mediterranean dietary pattern shown in Figure 1 revealed an inverse association for fruit consumption (RR: 0.93, 95% CI 0.89 to 0.97, I2 = 60%, n = 13 studies), vegetable intake (RR: 0.96, 95% CI 0.93 to 0.98, I2 = 0%, n = 14 studies), whole grain intake (RR: 0.91, 95% CI 0.87 to 0.95, I2 = 31%, n = 9 studies), and moderate alcohol consumption (within the range) (RR: 0.89, 95% CI 0.85 to 0.93), compared to higher intakes and cancer risk. No significant associations were observed for intakes of cereals, dairy, fish, legumes, meat, nuts, or olive oil (Figure 1).
3.4. Publication Bias
The Egger’s linear regression tests provided no evidence for a publication bias for overall cancer mortality (p = 0.86), breast cancer (p = 0.39), and colorectal cancer (p = 0.14), following comparison of the highest vs. lowest adherence to MedD category (Supplementary Materials Figures S21–S23). Funnel plots were only generated when at least 10 studies were available for a comparison. The funnel plots for risk of overall cancer mortality as well as risk of breast and colorectal cancer indicate moderate asymmetry, suggesting that publication bias cannot be completely excluded as a factor of influence on the present meta-analysis (Supplementary Materials Figures S21–S23).
4. Discussion
Following the synthesis of data from RCTs as well as cohort and case-control studies in the present systematic review, strongest adherence to a MedD was inversely associated with cancer mortality and risk of colorectal, breast, gastric, liver, head and neck, gallbladder, and biliary tract cancer. No significant associations could be observed with respect to other types of cancer and for cancer survivors. Considering dietary patterns instead of single nutrients or foods appears to have advantages in every respect. Foods are not consumed in separation and their health-related effects are additive or even synergistic [125]. Consequently, the Greek cohort of the EPIC study revealed that the inverse association between adherence to a MedD and cancer risk is not due to any single component of this diet but rather an effect of the complete pattern [126]. Contradictory to these observations, we could show significant inverse correlations between specific food groups typical for a MedD pattern (i.e., alcohol in moderate amounts, fruits, vegetables, and whole grains) and overall cancer risk (see Figure 1). In addition, a trend for potentially beneficial effects was detected for dairy, fish, and nuts, while meat pointed towards deleterious mechanisms. Fruits and vegetables contain numerous components known to have favorable effects on inflammatory, cellular redox, as well as metabolic processes and endothelial function, which might add up to their tumor-protective impact [127,128]. In addition, regular consumption of fruits and vegetables facilitates weight management in overweight subjects to counter obesity as a risk factor for cancer [129]. Whole grain products contain phytic acid, resistant starch, and soluble fiber, which are able to bind and neutralize potentially carcinogenic compounds in food [130]. An inverse association between whole grain intake and cancer risk was described in other meta-analyses as well [131,132]. Dairy products are included in the MedD pattern as a detrimental component. However, evidence regarding their health effects, especially for cancer, is controversial. A recent meta-analysis suggested dairy products are associated with a reduced risk for colorectal cancer risk [133], whereas a higher risk of prostate cancer has been reported [134]. Moreover, consumption of fermented dairy products was associated with a decreased risk to become obese or diabetic [135,136]. The health-promoting effects of dairy products might be explained by their high content of calcium, vitamins, and protein. Inverse associations between fish intake and all-cause as well as cancer mortality could be observed in various meta-analyses [137,138,139,140]. With respect to mechanisms, growth inhibitory, pro-apoptotic or anti-angiogenic effects can be attributed to the high amount of n-3 fatty acids present in fish [141,142]. Tree nuts contain anti-inflammatory, anti-oxidative, and endothelium-protective substances such as fiber, mono- and polyunsaturated fatty acids, or secondary plant metabolites which might prevent tumor pathogenesis and progression [143]. A significant cancer-protective effect of nuts could be demonstrated in a recent meta-analysis by Aune et al. [144]. Unfavorable effects of (red) meat and processed meat products might be due to ingredients promoting pro-inflammatory and pro-oxidative metabolic processes, e.g., nitrosamines, iron, or saturated fatty acids. A positive association between consumption of red meat and all-cause mortality could be observed in prospective cohorts from Europe and the US [145,146].
A specific and controversial “ingredient” of a MedD is ethanol, usually represented in the form of red wine. In some of the assessment indices mentioned, the highest rating/level of adherence could only be achieved when alcohol is consumed on a daily basis in moderate amounts. Ethanol is considered as a carcinogen in humans by the Agency for Research on Cancer [147]. The WCRF report summarizes alcoholic beverages as a risk factor in the development of different carcinomas (e.g., mouth, pharynx, larynx, esophagus, liver, colorectal, breast in pre- and post-menopause), with grades of evidence ranging between “convincing” and “probable”, respectively [129]. In some studies, consumption of alcoholic beverages even in low to moderate amounts was associated with an increased risk of colorectal, liver, and breast cancer as well as carcinomas of the larynx, pharynx, and esophagus [148]. Although red wine contains a number of potential protective ingredients such as anti-oxidative polyphenols, its beneficial role regarding malignant diseases is discussed controversially, e.g., with respect to non-Hodgkin’s lymphoma, renal cell carcinoma, breast cancer, or thyroid cancer [149,150,151,152]. When assessing the effects of a MedD on health and disease, one should keep in mind that the different scores for this dietary pattern may include alcoholic beverages. However, adherence to a MedD is usually defined by categories classified according to pre-defined cut off points. Thus, individuals in the highest categories cannot be discriminated according to their consumption of alcoholic beverages. Therefore, at present, it seems to be impossible to make an unequivocal statement on the effects of alcohol consumption regarding tumor pathogenesis. It seems pointless to recommend moderate alcohol consumption to hitherto abstinent individuals, especially cancer survivors.
Taken together, these data provide evidence that the combination of food groups in order to compose a pattern corresponding to a MedD exerts benefits with respect to tumor pathogenesis. However, it remains difficult to define the MedD as a distinct pattern. According to Simopoulos, the term “Mediterranean diet” is even misleading, since there is no clear-cut definition of a MedD but rather a number of variations based on different cultural, religious, ethnical, and economical versions of this regimen practiced by the populations of countries bordering the Mediterranean Sea [153]. Frequently used indices to assess the adherence to a MedD are the ones by Trichopoulou [36], the modified MedD index by the same group [154], the alternate Mediterranean Diet index [37], or the relative Mediterranean Diet index [85]. The initial three indices chose gender-specific medians of intake of relevant food groups as cutoff-points. It seems obvious that cutoff-points defined by medians vary between different populations, leading to an almost indefinite number of MedD subtypes. As a result, it will become impossible to differentiate between preferable and dissenting intakes [155]. Moreover, determination of the components of a MedD is inconsistent between different epidemiological studies. The characteristics of a MedD have changed considerably since the 1960s. Taking into account only some of its constituents does not justify categorization as a MedD pattern [156]. Thus, assessing the components of a MedD with respect to their potential tumor-preventive properties is subject to a number of prior conditions. It has to be noted that a large number of studies enrolled in the present systematic review fulfill these requirements, such as the special consideration of whole-grain products in the cereals category [37,74,104,110,111,112,113] or of extra virgin olive oil as the predominant provider of fat [85]. On the other hand, the protective effects of olive oil are most likely due to its content of polyphenols as well as their interactions [157]. Because of manufacturing conditions, not all of these compounds are present in every brand of olive oil, not even in extra virgin olive oil varieties [158]. Additionally, most studies measured intake of alcoholic beverages without special consideration of red wine (exceptions, e.g., [74,113]). For future assessments of a MedD it might be helpful to use a literature-based score implementing portions of each food group to achieve a pre-defined score such as the one suggested by Sofi et al. [30]. In addition, it might be helpful to explore linear trends via dose-response analyses as well as possible non-linear associations as has recently been done for the relation between 12 food groups and risk of type 2 diabetes mellitus [136].
Most of the data synthesized meta-analytically in the present systematic review were derived from epidemiological studies performed in either the US or European countries. These countries differ regarding their respective data on cancer prevalence, while at the same time, data from other countries are missing [159]. Additional to differences in adherence to varying dietary patterns, country-specific data may be explained by genetic factors, geographic features, or mixed exposures to carcinogens. The different manifestation of harmful and beneficial determinants in single countries might contribute to both over- as well as underestimation of the effects of a MedD. In some studies, the inverse association between adherence to a MedD and risk of tobacco-related cancers was significantly more pronounced in the subgroup of active smokers [78,160].
The validity of our results is further limited by methodological shortcomings of some of the studies enrolled in the present systematic review. The most common tool to assess a dietary regimen in observational studies is the food frequency questionnaire. It is an established and cost-effective instrument, however, with a number of disadvantages. Lesser number of items and short survey periods might not necessarily represent a dietary pattern with impact on chronic diseases and mortality. However, most of the included studies did assess the whole diet via FFQ over a period of more than 12 months.
Another limitation was the lopsided availability of studies by type of cancer. The most frequently investigated tumor localizations in the present study were breast, colorectal, prostate, and head-and-neck cancer, while other types of cancer such as lung or esophageal cancer were explored to a lesser extent. Taken together, these limitations might at least in part explain the considerable heterogeneity present in our systematic review (Table 2).
The observed high statistical heterogeneity for cancer mortality was related to the different definitions for MedD pattern. Additional analyses indicated lower levels of heterogeneity when studies were grouped according to similar definitions of a MedD pattern (e.g., alternate MedD, or traditional MedD). The high levels of heterogeneity observed for colorectal cancer risk in the main analysis could not be confirmed for cohort studies in the stratified analysis, and were mainly driven by one large case-control study.
Due to the low number of studies available for several cancer types, we were not able to investigate properly potential sources of heterogeneity. However, statistical heterogeneity might be related to differences in adjustment factors, as well as heterogeneous definition of the MedD.
To some degree, our results might depend on residual confounders. Hypothesis-Driven dietary patterns [161] represent one aspect of a multidimensional lifestyle complex including other factors such as exercise, smoking behavior, and alcohol consumption [162]. Although the results of the studies are most often adjusted for these factors via multivariate analyses, we cannot exclude potential confounders as another limitation affecting our results. The benefits of a MedD were found to be depending on cohort characteristics such as smoking behavior [85], age groups [37,85], hormonal status [37,116], or gender [89,94].
Strengths of the present study are the extensive literature research with strict adherence to quality standards set by PRISMA guidelines. Data were synthesized predominantly from observational studies enrolling a high number of participants, which, in some cases, may compensate for the low number of studies investigating specific tumor localizations.
5. Conclusions
In conclusion, the present update of our systematic review and meta-analyses provided additional important evidence for a beneficial effect of high adherence to MedD with respect to primary prevention overall cancer risk and specific types of cancer, especially colorectal cancer. These observed beneficial effects are mainly driven by higher intakes of fruits, vegetables, and whole grains. Moreover, we report for the first time a small decrease in breast cancer risk (6%) with the pooling seven cohort studies. To further elucidate the relationship between Mediterranean dietary patterns and cancer types, future studies should adopt a precise definition of a MedD.
Supplementary Materials
The following are available online at www.mdpi.com/2072-6643/9/10/1063/s1.
Author Contributions
L.S., C.S., and G.H. collected the data. L.S. and G.H. wrote the first draft with contributions from C.S. and C.G. All authors reviewed and commented on subsequent drafts of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Search strategy for PubMed: (“Mediterranean diet” OR “Mediterranean” OR “diet” OR “dietary pattern” OR “dietary score” OR “dietary adherence”) AND (“cancer” OR “neoplasm” OR “neoplastic disease” OR “survivors” OR “recurrence”) AND (“prospective” OR “follow- up” OR “cohort” OR “longitudinal”).
References
- Stewart, B.W.; Bray, F.; Forman, D.; Ohgaki, H.; Straif, K.; Ullrich, A.; Wild, C.P. Cancer prevention as part of precision medicine: ‘Plenty to be done’. Carcinogenesis 2016, 37, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Tyrovolas, S.; Panagiotakos, D.B. The role of Mediterranean type of diet on the development of cancer and cardiovascular disease, in the elderly: A systematic review. Maturitas 2010, 65, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, Z.; Peckham, C.S.; Ades, A.E. Changing prevalence of juvenile-onset diabetes mellitus. Lancet 1988, 2, 88–90. [Google Scholar] [CrossRef]
- Ligibel, J.A.; Alfano, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Burger, R.A.; Chlebowski, R.T.; Fabian, C.J.; Gucalp, A.; Hershman, D.L.; Hudson, M.M.; et al. American Society of Clinical Oncology position statement on obesity and cancer. J. Clin. Oncol. 2014, 32, 3568–3574. [Google Scholar] [CrossRef] [PubMed]
- Anand, P.; Kunnumakkara, A.B.; Sundaram, C.; Harikumar, K.B.; Tharakan, S.T.; Lai, O.S.; Sung, B.; Aggarwal, B.B. Cancer is a preventable disease that requires major lifestyle changes. Pharm. Res. 2008, 25, 2097–2116. [Google Scholar] [CrossRef] [PubMed]
- WCRF. World Cancer Research Fund International. Continuous Update Project (Cup). 2017. Available online: http://www.wcrf.org/int/research-we-fund/continuous-update-project-cup (accessed on 20 July 2017).
- Heller, M.C.; Keoleian, G.A.; Willett, W.C. Toward a life cycle-based, diet-level framework for food environmental impact and nutritional quality assessment: A critical review. Environ. Sci. Technol. 2013, 47, 12632–12647. [Google Scholar] [CrossRef] [PubMed]
- Milner, J.A. Molecular targets for bioactive food components. J. Nutr. 2004, 134, 2492s–2498s. [Google Scholar] [PubMed]
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K.; International Agency for Research on Cancer Monograph Working Group. Carcinogenicity of consumption of red and processed meat. Lancet Oncol. 2015, 16, 1599–1600. [Google Scholar] [CrossRef]
- Bagnardi, V.; Rota, M.; Botteri, E.; Tramacere, I.; Islami, F.; Fedirko, V.; Scotti, L.; Jenab, M.; Turati, F.; Pasquali, E.; et al. Alcohol consumption and site-specific cancer risk: A comprehensive dose-response meta-analysis. Br. J. Cancer 2015, 112, 580–593. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, M. The second World Cancer Research Fund/American Institute for Cancer Research expert report. Food, nutrition, physical activity, and the prevention of cancer: A global perspective. Proc. Nutr. Soc. 2008, 67, 253–256. [Google Scholar] [CrossRef] [PubMed]
- Mullan, F. Seasons of survival: Reflections of a physician with cancer. N. Engl. J. Med. 1985, 313, 270–273. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Rowland, J.H.; Kent, E.E.; Forsythe, L.P.; Loge, J.H.; Hjorth, L.; Glaser, A.; Mattioli, V.; Fossa, S.D. Cancer survivorship research in Europe and the United states: Where have we been, where are we going, and what can we learn from each other? Cancer 2013, 119 (Suppl. 11), 2094–2108. [Google Scholar] [CrossRef] [PubMed]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Collins, C.E.; Young, A.F.; Hodge, A. Diet quality is associated with higher nutrient intake and self-rated health in mid-aged women. J. Am. Coll. Nutr. 2008, 27, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.R.; Gross, M.D.; Tapsell, L.C. Food synergy: An operational concept for understanding nutrition. Am. J. Clin. Nutr. 2009, 89, 1543S–1548S. [Google Scholar] [CrossRef] [PubMed]
- Edefonti, V.; Randi, G.; La Vecchia, C.; Ferraroni, M.; Decarli, A. Dietary patterns and breast cancer: A review with focus on methodological issues. Nutr. Rev. 2009, 67, 297–314. [Google Scholar] [CrossRef] [PubMed]
- Keys, A. Mediterranean diet and public health: Personal reflections. Am. J. Clin. Nutr. 1995, 61, 1321S–1323S. [Google Scholar] [PubMed]
- Keys, A.; Menotti, A.; Karvonen, M.J.; Aravanis, C.; Blackburn, H.; Buzina, R.; Djordjevic, B.S.; Dontas, A.S.; Fidanza, F.; Keys, M.H. The diet and 15-year death rate in the Seven countries study. Am. J. Epidemiol. 1986, 124, 903–915. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Missbach, B.; Konig, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Mediterranean dietary pattern, inflammation and endothelial function: A systematic review and meta-analysis of intervention trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef] [PubMed]
- Fidanza, F.; Alberti, A.; Fruttini, D. The Nicotera diet: The reference Italian Mediterranean diet. World Rev. Nutr. Diet. 2005, 95, 115–121. [Google Scholar] [PubMed]
- Fidanza, F.; Alberti, A.; Lanti, M.; Menotti, A. Mediterranean Adequacy Index: Correlation with 25-year mortality from coronary heart disease in the Seven countries study. Nutr. Metab. Cardiovasc. Dis. 2004, 14, 254–258. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Monounsaturated fatty acids, olive oil and health status: A systematic review and meta-analysis of cohort studies. Lipids Health Dis. 2014, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C.; Sacks, F.; Trichopoulou, A.; Drescher, G.; Ferro-Luzzi, A.; Helsing, E.; Trichopoulos, D. Mediterranean diet pyramid: A cultural model for healthy eating. Am. J. Clin. Nutr. 1995, 61, 1402S–1406S. [Google Scholar] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: A systematic review and meta-analysis of observational studies. Int. J. Cancer 2014, 135, 1884–1897. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Adherence to mediterranean diet and risk of cancer: An updated systematic review and meta-analysis of observational studies. Cancer Med. 2015, 4, 1933–1947. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769–2782. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G. Does a Mediterranean-type diet reduce cancer risk? Curr. Nutr. Rep. 2016, 5, 9–17. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M.; Salen, P.; Martin, J.L.; Monjaud, I.; Boucher, P.; Mamelle, N. Mediterranean dietary pattern in a randomized trial: Prolonged survival and possible reduced cancer rate. Arch. Intern. Med. 1998, 158, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Toledo, E.; Salas-Salvado, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fito, M.; Hu, F.B.; Aros, F.; et al. Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in the PREDIMED trial: A randomized clinical trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Estruch, R.; Ros, E.; Salas-Salvado, J. Primary prevention of cardiovascular disease with a mediterranean diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef] [PubMed]
- De Lorgeril, M.; Renaud, S.; Mamelle, N.; Salen, P.; Martin, J.L.; Monjaud, I.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Hu, F.B.; McCullough, M.L.; Newby, P.K.; Willett, W.C.; Holmes, M.D. Diet quality is associated with the risk of estrogen receptor-negative breast cancer in postmenopausal women. J. Nutr. 2006, 136, 466–472. [Google Scholar] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean food pattern predicts the prevalence of hypertension, hypercholesterolemia, diabetes and obesity, among healthy adults; the accuracy of the MedDietscore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Menotti, A.; Alberti-Fidanza, A.; Fidanza, F.; Lanti, M.; Fruttini, D. Factor analysis in the identification of dietary patterns and their predictive role in morbid and fatal events. Public Health Nutr. 2012, 15, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Murtaugh, M.A.; Sweeney, C.; Giuliano, A.R.; Herrick, J.S.; Hines, L.; Byers, T.; Baumgartner, K.B.; Slattery, M.L. Diet patterns and breast cancer risk in hispanic and non-Hispanic white women: The Four-Corners Breast Cancer Study. Am. J. Clin. Nutr. 2008, 87, 978–984. [Google Scholar] [PubMed]
- Cottet, V.; Touvier, M.; Fournier, A.; Touillaud, M.S.; Lafay, L.; Clavel-Chapelon, F.; Boutron-Ruault, M.C. Postmenopausal breast cancer risk and dietary patterns in the E3N-EPIC prospective cohort study. Am. J. Epidemiol. 2009, 170, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Bessaoud, F.; Tretarre, B.; Daures, J.P.; Gerber, M. Identification of dietary patterns using two statistical approaches and their association with breast cancer risk: A case-control study in Southern France. Ann. Epidemiol. 2012, 22, 499–510. [Google Scholar] [CrossRef] [PubMed]
- Castelló, A.; Boldo, E.; Pérez-Gómez, B.; Lope, V.; Altzibar, J.M.; Martín, V.; Castaño-Vinyals, G.; Guevara, M.; Dierssen-Sotos, T.; Tardón, A.; et al. Adherence to the Western, Prudent and Mediterranean dietary patterns and breast cancer risk: MCC-Spain study. Maturitas 2017, 103, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Castelló, A.; Boldo, E.; Amiano, P.; Castaño-Vinyals, G.; Aragonés, N.; Gómez-Acebo, I.; Peiró, R.; Jimenez-Moleón, J.J.; Alguacil, J.; Tardón, A.; et al. Mediterranean dietary pattern is associated to low risk of aggressive prostate cancer: MCC-Spain study. J. Urol. 2017. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, M.; Davey, S.G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Stovold, E.; Beecher, D.; Foxlee, R.; Noel-Storr, A. Study flow diagrams in cochrane systematic review updates: An adapted PRISMA flow diagram. Syst. Rev. 2014, 3, 54. [Google Scholar] [CrossRef] [PubMed]
- Anic, G.M.; Park, Y.; Subar, A.F.; Schap, T.E.; Reedy, J. Index-based dietary patterns and risk of lung cancer in the NIH-AARP Diet and Health Study. Eur. J. Clin. Nutr. 2016, 70, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Dugue, P.A.; Hodge, A.M.; Brinkman, M.T.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; Hopper, J.L.; English, D.R.; Milne, R.L.; Giles, G.G. Association between selected dietary scores and the risk of urothelial cell carcinoma: A prospective cohort study. Int. J. Cancer 2016, 139, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Haridass, V. Diet Quality Scores and Risk of Incident Breast Cancer in the California Teachers Study 2015. (Dissertation). Available online: http://escholarship.Org/uc/item/87t2942b (accessed on 25 July 2017).
- Hirko, K.A.; Willett, W.C.; Hankinson, S.E.; Rosner, B.A.; Beck, A.H.; Tamimi, R.M.; Eliassen, A.H. Healthy dietary patterns and risk of breast cancer by molecular subtype. Breast Cancer Res Treat. 2016, 155, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Hodge, A.M.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; English, D.R.; Giles, G.G.; Severi, G. Dietary Inflammatory Index, Mediterranean diet score, and lung cancer: A prospective study. Cancer Causes Control 2016, 27, 907–917. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Harmon, B.E.; Ollberding, N.J.; Wilkens, L.R.; Monroe, K.R.; Kolonel, L.N.; Le Marchand, L.; Boushey, C.J.; Maskarinec, G. Among 4 diet quality indexes, only the Alternate Mediterranean diet score is associated with better colorectal cancer survival and only in african american women in the Multiethnic cohort. J. Nutr. 2016, 146, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Hakansson, N.; Wolk, A. Healthy dietary patterns and incidence of biliary tract and gallbladder cancer in a prospective study of women and men. Eur. J. Cancer 2017, 70, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Lassale, C.; Gunter, M.J.; Romaguera, D.; Peelen, L.M.; Van der Schouw, Y.T.; Beulens, J.W.; Freisling, H.; Muller, D.C.; Ferrari, P.; Huybrechts, I.; et al. Diet quality scores and prediction of all-cause, cardiovascular and cancer mortality in a pan-european cohort study. PLoS ONE 2016, 11, e0159025. [Google Scholar] [CrossRef] [PubMed]
- Maisonneuve, P.; Shivappa, N.; Hebert, J.R.; Bellomi, M.; Rampinelli, C.; Bertolotti, R.; Spaggiari, L.; Palli, D.; Veronesi, G.; Gnagnarella, P. Dietary inflammatory index and risk of lung cancer and other respiratory conditions among heavy smokers in the COMOS screening study. Eur. J. Nutr. 2016, 55, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Molina-Montes, E.; Sanchez, M.J.; Buckland, G.; Bueno-de-Mesquita, H.B.; Weiderpass, E.; Amiano, P.; Wark, P.A.; Kuhn, T.; Katzke, V.; Huerta, J.M.; et al. Mediterranean diet and risk of pancreatic cancer in the European Prospective Investigation into Cancer and Nutrition cohort. Br. J. Cancer 2017, 116, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Boushey, C.J.; Wilkens, L.R.; Haiman, C.A.; Le Marchand, L. High-quality diets associate with reduced risk of colorectal cancer: Analyses of diet quality indexes in the Multiethnic cohort. Gastroenterology 2017, 153, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Van den Brandt, P.A.; Schulpen, M. Mediterranean diet adherence and risk of postmenopausal breast cancer: Results of a cohort study and meta-analysis. Int. J. Cancer 2017, 140, 2220–2231. [Google Scholar] [CrossRef] [PubMed]
- Vargas, A.J.; Neuhouser, M.L.; George, S.M.; Thomson, C.A.; Ho, G.Y.; Rohan, T.E.; Kato, I.; Nassir, R.; Hou, L.; Manson, J.E. Diet quality and colorectal cancer risk in the Women’s Health Initiative observational study. Am. J. Epidemiol. 2016, 184, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Whalen, K.A.; Judd, S.; McCullough, M.L.; Flanders, W.D.; Hartman, T.J.; Bostick, R.M. Paleolithic and Mediterranean diet pattern scores are inversely associated with all-cause and cause-specific mortality in adults. J. Nutr. 2017, 147, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Butler, L.M.; Wu, A.H.; Wang, R.; Koh, W.P.; Yuan, J.M.; Yu, M.C. A vegetable-fruit-soy dietary pattern protects against breast cancer among postmenopausal Singapore Chinese women. Am. J. Clin. Nutr. 2010, 91, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.; Evans, C.; Cade, J.; Hancock, N.; Greenwood, D. The Mediterranean diet and risk of colorectal cancer in the UK Women’s cohort study. Int. J. Epidemiol. 2017. [Google Scholar] [CrossRef]
- Askari, F.; Beyzaei, B.; Tehrani, A.; Parizi, M.K.; Mirshekarlou, E.N.; Rashidkhani, B. Adherence to Mediterranean-style dietary pattern and risk of prostate cancer: A case-control study in Iran. Pak. J. Nutr. 2016, 15, 305–311. [Google Scholar]
- Campagna, M.; Cocco, P.; Zucca, M.; Angelucci, E.; Gabbas, A.; Latte, G.C.; Uras, A.; Rais, M.; Sanna, S.; Ennas, M.G. Risk of lymphoma subtypes and dietary habits in a Mediterranean area. Cancer Epidemiol. 2015, 39, 1093–1098. [Google Scholar] [CrossRef] [PubMed]
- Giraldi, L.; Panic, N.; Cadoni, G.; Boccia, S.; Leoncini, E. Association between Mediterranean diet and head and neck cancer: Results of a large case-control study in Italy. Eur. J. Cancer Prev. 2017, 26, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Guercio, V.; Bosetti, C.; Negri, E.; Serraino, D.; Giacosa, A.; Montella, M.; La Vecchia, C.; Tavani, A. Mediterranean diet and colorectal cancer risk: A pooled analysis of three Italian case-control studies. Br. J. Cancer 2016, 115, 862–865. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, J.; Giraldi, L.; Arzani, D.; Pastorino, R.; Biondi, A.; Persiani, R.; Boccia, S.; Leoncini, E. Adherence to Mediterranean diet and risk of gastric cancer: Results of a case-control study in Italy. Eur. J. Cancer. Prev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Bravi, F.; Polesel, J.; Bosetti, C.; Negri, E.; Garavello, W.; Taborelli, M.; Serraino, D.; Libra, M.; Montella, M.; et al. Adherence to the Mediterranean diet and nasopharyngeal cancer risk in Italy. Cancer Causes Control 2017, 28, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lin, X.L.; Fan, Y.Y.; Liu, Y.T.; Zhang, X.L.; Lu, Y.K.; Xu, C.H.; Chen, Y.M. Diet quality scores and risk of nasopharyngeal carcinoma in Chinese adults: A case-control study. Nutrients 2016, 8, 112. [Google Scholar] [CrossRef] [PubMed]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: The HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Tognon, G.; Nilsson, L.M.; Lissner, L.; Johansson, I.; Hallmans, G.; Lindahl, B.; Winkvist, A. The Mediterranean diet score and mortality are inversely associated in adults living in the subarctic region. J. Nutr. 2012, 142, 1547–1553. [Google Scholar] [CrossRef] [PubMed]
- Nkondjock, A.; Ghadirian, P. Diet quality and BRCA-associated breast cancer risk. Breast Cancer Res. Treat. 2007, 103, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Ax, E.; Garmo, H.; Grundmark, B.; Bill-Axelson, A.; Holmberg, L.; Becker, W.; Zethelius, B.; Cederholm, T.; Sjogren, P. Dietary patterns and prostate cancer risk: Report from the population based ULSAM cohort study of Swedish men. Nutr. Cancer 2014, 66, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Bamia, C.; Lagiou, P.; Buckland, G.; Grioni, S.; Agnoli, C.; Taylor, A.J.; Dahm, C.C.; Overvad, K.; Olsen, A.; Tjonneland, A.; et al. Mediterranean diet and colorectal cancer risk: Results from a European cohort. Eur. J. Epidemiol. 2013, 28, 317–328. [Google Scholar] [CrossRef] [PubMed]
- Couto, E.; Boffetta, P.; Lagiou, P.; Ferrari, P.; Buckland, G.; Overvad, K.; Dahm, C.C.; Tjonneland, A.; Olsen, A.; Clavel-Chapelon, F.; et al. Mediterranean dietary pattern and cancer risk in the EPIC cohort. Br. J. Cancer 2011, 104, 1493–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckland, G.; Travier, N.; Cottet, V.; Gonzalez, C.A.; Lujan-Barroso, L.; Agudo, A.; Trichopoulou, A.; Lagiou, P.; Trichopoulos, D.; Peeters, P.H.; et al. Adherence to the Mediterranean diet and risk of breast cancer in the European Prospective Investigation into Cancer and Nutrition cohort study. Int. J. Cancer 2013, 132, 2918–2927. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Agudo, A.; Travier, N.; Huerta, J.M.; Cirera, L.; Tormo, M.J.; Navarro, C.; Chirlaque, M.D.; Moreno-Iribas, C.; Ardanaz, E.; et al. Adherence to the Mediterranean diet reduces mortality in the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition (Epic-spain). Br. J. Nutr. 2011, 106, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Couto, E.; Sandin, S.; Lof, M.; Ursin, G.; Adami, H.O.; Weiderpass, E. Mediterranean dietary pattern and risk of breast cancer. PLoS ONE 2013, 8, e55374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Gonzalez, M.A.; Guillen-Grima, F.; De Irala, J.; Ruiz-Canela, M.; Bes-Rastrollo, M.; Beunza, J.J.; Lopez del Burgo, C.; Toledo, E.; Carlos, S.; Sanchez-Villegas, A. The Mediterranean diet is associated with a reduction in premature mortality among middle-aged adults. J. Nutr. 2012, 142, 1672–1678. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Turati, F.; Dal Pont, A.; Ferraroni, M.; Polesel, J.; Negri, E.; Serraino, D.; Talamini, R.; La Vecchia, C.; Zeegers, M.P. The role of Mediterranean diet on the risk of pancreatic cancer. Br. J. Cancer 2013, 109, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Moller, E.; Galeone, C.; Andersson, T.M.; Bellocco, R.; Adami, H.O.; Andren, O.; Gronberg, H.; La Vecchia, C.; Mucci, L.A.; Balter, K. Mediterranean diet score and prostate cancer risk in a Swedish population-based case-control study. J. Nutr. Sci. 2013, 2, e15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckland, G.; Agudo, A.; Lujan, L.; Jakszyn, P.; Bueno-de-Mesquita, H.B.; Palli, D.; Boeing, H.; Carneiro, F.; Krogh, V.; Sacerdote, C.; et al. Adherence to a Mediterranean diet and risk of gastric adenocarcinoma within the European Prospective Investigation into Cancer and Nutrition cohort study. Am. J. Clin. Nutr. 2010, 91, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Praud, D.; Bertuccio, P.; Bosetti, C.; Turati, F.; Ferraroni, M.; La Vecchia, C. Adherence to the Mediterranean diet and gastric cancer risk in Italy. Int. J. Cancer 2014, 134, 2935–2941. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.E.; Taylor, E.F.; Burley, V.J.; Greenwood, D.C. Does the Mediterranean dietary pattern or the Healthy Diet Index influence the risk of breast cancer in a large British cohort of women? Eur. J Clin. Nutr. 2011, 65, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Lagiou, P.; Trichopoulos, D.; Sandin, S.; Lagiou, A.; Mucci, L.; Wolk, A.; Weiderpass, E.; Adami, H.O. Mediterranean dietary pattern and mortality among young women: A cohort study in Sweden. Br. J. Nutr. 2006, 96, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Dixon, L.B.; Subar, A.F.; Peters, U.; Weissfeld, J.L.; Bresalier, R.S.; Risch, A.; Schatzkin, A.; Hayes, R.B. Adherence to the USDA food guide, DASH eating plan, and Mediterranean dietary pattern reduces risk of colorectal adenoma. J. Nutr. 2007, 137, 2443–2450. [Google Scholar] [PubMed]
- Wu, A.H.; Yu, M.C.; Tseng, C.C.; Stanczyk, F.Z.; Pike, M.C. Dietary patterns and breast cancer risk in Asian American women. Am. J. Clin. Nutr. 2009, 89, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Hu, F.B.; Wu, K.; Chiuve, S.E.; Fuchs, C.S.; Giovannucci, E. The Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets and colorectal cancer. Am. J. Clin. Nutr. 2010, 92, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Kenfield, S.A.; DuPre, N.; Richman, E.L.; Stampfer, M.J.; Chan, J.M.; Giovannucci, E.L. Mediterranean diet and prostate cancer risk and mortality in the Health Professionals Follow-up Study. Eur. Urol. 2014, 65, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Park, Y.; Wu, J.W.; Ren, J.S.; Goldstein, A.M.; Taylor, P.R.; Hollenbeck, A.R.; Freedman, N.D.; Abnet, C.C. Index-based dietary patterns and risk of esophageal and gastric cancer in a large cohort study. Clin. Gastroenterol. Hepatol. 2013, 11, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Mitrou, P.N.; Krebs-Smith, S.M.; Wirfalt, E.; Flood, A.; Kipnis, V.; Leitzmann, M.; Mouw, T.; Hollenbeck, A.; Schatzkin, A.; et al. Index-based dietary patterns and risk of colorectal cancer: The NIH-AARP Diet and Health Study. Am. J. Epidemiol. 2008, 168, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Mitrou, P.N.; Kipnis, V.; Thiebaut, A.C.; Reedy, J.; Subar, A.F.; Wirfalt, E.; Flood, A.; Mouw, T.; Hollenbeck, A.R.; Leitzmann, M.F.; et al. Mediterranean dietary pattern and prediction of all-cause mortality in a US population: Results from the NIH-AARP Diet and Health Study. Arch. Int. Med. 2007, 167, 2461–2468. [Google Scholar] [CrossRef] [PubMed]
- Samoli, E.; Lagiou, A.; Nikolopoulos, E.; Lagogiannis, G.; Barbouni, A.; Lefantzis, D.; Trichopoulos, D.; Brennan, P.; Lagiou, P. Mediterranean diet and upper aerodigestive tract cancer: The Greek segment of the Alcohol-Related cancers and Genetic Susceptibility in Europe study. Br. J. Nutr. 2010, 104, 1369–1374. [Google Scholar] [CrossRef] [PubMed]
- Bosire, C.; Stampfer, M.J.; Subar, A.F.; Park, Y.; Kirkpatrick, S.I.; Chiuve, S.E.; Hollenbeck, A.R.; Reedy, J. Index-based dietary patterns and the risk of prostate cancer in the NIH-AARP Diet and Health Study. Am. J. Epidemiol. 2013, 177, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Cottet, V.; Bonithon-Kopp, C.; Kronborg, O.; Santos, L.; Andreatta, R.; Boutron-Ruault, M.C.; Faivre, J. Dietary patterns and the risk of colorectal adenoma recurrence in a European intervention trial. Eur. J. Cancer Prev. 2005, 14, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Demetriou, C.A.; Hadjisavvas, A.; Loizidou, M.A.; Loucaides, G.; Neophytou, I.; Sieri, S.; Kakouri, E.; Middleton, N.; Vineis, P.; Kyriacou, K. The Mediterranean dietary pattern and breast cancer risk in Greek-cypriot women: A case-control study. BMC Cancer 2012, 12, 113. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Gallus, S.; Trichopoulou, A.; Talamini, R.; Franceschi, S.; Negri, E.; La Vecchia, C. Influence of the Mediterranean diet on the risk of cancers of the upper aerodigestive tract. Cancer Epidemiol. Biomark. Prev. 2003, 12, 1091–1094. [Google Scholar]
- Kontou, N.; Psaltopoulou, T.; Soupos, N.; Polychronopoulos, E.; Xinopoulos, D.; Linos, A.; Panagiotakos, D.B. Metabolic syndrome and colorectal cancer: The protective role of Mediterranean diet-a case-control study. Angiology 2012, 63, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Buckland, G.; Ros, M.M.; Roswall, N.; Bueno-de-Mesquita, H.B.; Travier, N.; Tjonneland, A.; Kiemeney, L.A.; Sacerdote, C.; Tumino, R.; Ljungberg, B.; et al. Adherence to the Mediterranean diet and risk of bladder cancer in the EPIC cohort study. Int. J. Cancer 2014, 134, 2504–2511. [Google Scholar] [CrossRef] [PubMed]
- Cuenca-Garcia, M.; Artero, E.G.; Sui, X.; Lee, D.C.; Hebert, J.R.; Blair, S.N. Dietary indices, cardiovascular risk factors and mortality in middle-aged adults: Findings from the Aerobics Center Longitudinal Study. Ann. Epdemiol. 2014, 24, 297.e2–303.e2. [Google Scholar] [CrossRef] [PubMed]
- George, S.M.; Ballard-Barbash, R.; Manson, J.E.; Reedy, J.; Shikany, J.M.; Subar, A.F.; Tinker, L.F.; Vitolins, M.; Neuhouser, M.L. Comparing indices of diet quality with chronic disease mortality risk in postmenopausal women in the Women’s Health Initiative Observational Study: Evidence to inform national dietary guidance. Am. J. Epdemiol. 2014, 180, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Maisonneuve, P.; Bellomi, M.; Rampinelli, C.; Bertolotti, R.; Spaggiari, L.; Palli, D.; Veronesi, G. Red meat, Mediterranean diet and lung cancer risk among heavy smokers in the COSMOS screening study. Ann. Oncol. 2013, 24, 2606–2611. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; Kashambwa, R.; Sato, K.; Chiuve, S.E.; Fuchs, C.S.; Wu, K.; Giovannucci, E.; Ogino, S.; Hu, F.B.; Meyerhardt, J.A. Post diagnosis diet quality and colorectal cancer survival in women. PLoS ONE 2014, 9, e115377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.H.; Willett, W.C.; Fung, T.; Rosner, B.; Holmes, M.D. Diet quality indices and postmenopausal breast cancer survival. Nutr. Cancer 2011, 63, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Park, Y.; McGlynn, K.A.; Hollenbeck, A.R.; Taylor, P.R.; Goldstein, A.M.; Freedman, N.D. Index-based dietary patterns and risk of incident hepatocellular carcinoma and mortality from chronic liver disease in a prospective study. Hepatology 2014, 60, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Q.; Park, Y.; Wu, J.W.; Goldstein, A.M.; Taylor, P.R.; Hollenbeck, A.R.; Freedman, N.D.; Abnet, C.C. Index-based dietary patterns and risk of head and neck cancer in a large prospective study. Am. J. Clin. Nutr. 2014, 99, 559–566. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Garcia, E.; Rodriguez-Artalejo, F.; Li, T.Y.; Fung, T.T.; Li, S.; Willett, W.C.; Rimm, E.B.; Hu, F.B. The Mediterranean-style dietary pattern and mortality among men and women with cardiovascular disease. Am. J. Clin. Nutr. 2014, 99, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Reedy, J.; Krebs-Smith, S.M.; Miller, P.E.; Liese, A.D.; Kahle, L.L.; Park, Y.; Subar, A.F. Higher diet quality is associated with decreased risk of all-cause, cardiovascular disease, and cancer mortality among older adults. J. Nutr. 2014, 144, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Harmon, B.E.; Boushey, C.J.; Shvetsov, Y.B.; Ettienne, R.; Reedy, J.; Wilkens, L.R.; Le Marchand, L.; Henderson, B.E.; Kolonel, L.N. Associations of key diet-quality indexes with mortality in the Multiethnic Cohort: The Dietary Patterns Methods Project. Am. J. Clin. Nutr. 2015, 101, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Vormund, K.; Braun, J.; Rohrmann, S.; Bopp, M.; Ballmer, P.; Faeh, D. Mediterranean diet and mortality in Switzerland: An alpine paradox? Eur. J. Nutr. 2015, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Poole, E.M.; Terry, K.L.; Fung, T.T.; Rosner, B.A.; Willett, W.C.; Tworoger, S.S. A prospective cohort study of dietary indices and incidence of epithelial ovarian cancer. J. Ovarian Res. 2014, 7, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castello, A.; Pollan, M.; Buijsse, B.; Ruiz, A.; Casas, A.M.; Baena-Canada, J.M.; Lope, V.; Antolin, S.; Ramos, M.; Munoz, M.; et al. Spanish Mediterranean diet and other dietary patterns and breast cancer risk: Case-control EPIGEICAM study. Br. J. Cancer 2014, 111, 1454–1462. [Google Scholar] [CrossRef] [PubMed]
- Dalvi, T.B.; Canchola, A.J.; Horn-Ross, P.L. Dietary patterns, Mediterranean diet, and endometrial cancer risk. Cancer Causes Control 2007, 18, 957–966. [Google Scholar] [CrossRef] [PubMed]
- Grosso, G.; Biondi, A.; Galvano, F.; Mistretta, A.; Marventano, S.; Buscemi, S.; Drago, F.; Basile, F. Factors associated with colorectal cancer in the context of the Mediterranean diet: A case-control study. Nutr. Cancer 2014, 66, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Filomeno, M.; Bosetti, C.; Garavello, W.; Levi, F.; Galeone, C.; Negri, E.; La Vecchia, C. The role of a Mediterranean diet on the risk of oral and pharyngeal cancer. Br. J. Cancer 2014, 111, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Mourouti, N.; Kontogianni, M.D.; Papavagelis, C.; Plytzanopoulou, P.; Vassilakou, T.; Malamos, N.; Linos, A.; Panagiotakos, D.B. Adherence to the Mediterranean diet is associated with lower likelihood of breast cancer: A case-control study. Nutr. Cancer 2014, 66, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Pot, G.K.; Stephen, A.M.; Dahm, C.C.; Key, T.J.; Cairns, B.J.; Burley, V.J.; Cade, J.E.; Greenwood, D.C.; Keogh, R.H.; Bhaniani, A.; et al. Dietary patterns derived with multiple methods from food diaries and breast cancer risk in the UK Dietary Cohort Consortium. Eur. J. Clin. Nutr. 2014, 68, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Turati, F.; Trichopoulos, D.; Polesel, J.; Bravi, F.; Rossi, M.; Talamini, R.; Franceschi, S.; Montella, M.; Trichopoulou, A.; La Vecchia, C.; et al. Mediterranean diet and hepatocellular carcinoma. J. Hepatol. 2014, 60, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Whalen, K.A.; McCullough, M.; Flanders, W.D.; Hartman, T.J.; Judd, S.; Bostick, R.M. Paleolithic and Mediterranean diet pattern scores and risk of incident, sporadic colorectal adenomas. Am. J. Epidemiol. 2014, 180, 1088–1097. [Google Scholar] [CrossRef] [PubMed]
- George, S.M.; Ballard, R.; Shikany, J.M.; Crane, T.E.; Neuhouser, M.L. A prospective analysis of diet quality and endometrial cancer among 84,415 postmenopausal women in the Women’s Health Initiative. Ann. Epidemiol. 2015, 25, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Filomeno, M.; Bosetti, C.; Bidoli, E.; Levi, F.; Serraino, D.; Montella, M.; La Vecchia, C.; Tavani, A. Mediterranean diet and risk of endometrial cancer: A pooled analysis of three Italian case-control studies. Br. J. Cancer 2015, 112, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Kant, A.K. Dietary patterns and health outcomes. J. Am. Diet. Assoc. 2004, 104, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Benetou, V.; Trichopoulou, A.; Orfanos, P.; Naska, A.; Lagiou, P.; Boffetta, P.; Trichopoulos, D.; Cohort, G.E. Conformity to traditional Mediterranean diet and cancer incidence: The Greek EPIC cohort. Br. J. Cancer 2008, 99, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Boeing, H.; Bechthold, A.; Bub, A.; Ellinger, S.; Haller, D.; Kroke, A.; Leschik-Bonnet, E.; Muller, M.J.; Oberritter, H.; Schulze, M.; et al. Critical review: Vegetables and fruit in the prevention of chronic diseases. Eur. J. Nutr. 2012, 51, 637–663. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.H. Health-promoting components of fruits and vegetables in the diet. Adv. Nutr. 2013, 4, 384s–392s. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: A Global Perspective; AICR: Washington, DC, USA, 2007. [Google Scholar]
- Fardet, A. New hypotheses for the health-protective mechanisms of whole-grain cereals: What is beyond fibre? Nutr. Res. Rev. 2010, 23, 65–134. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Chan, D.S.; Lau, R.; Vieira, R.; Greenwood, D.C.; Kampman, E.; Norat, T. Dietary fibre, whole grains, and risk of colorectal cancer: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2011, 343, d6617. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: Systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef] [PubMed]
- Vieira, A.R.; Abar, L.; Chan, D.; Vingeliene, S.; Polemiti, E.; Stevens, C.; Greenwood, D.; Norat, T. Foods and beverages and colorectal cancer risk: A systematic review and meta-analysis of cohort studies, an update of the evidence of the WCRF-AICR Continuous Update Project. Ann. Oncol. 2017, 28, 1788–1802. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Navarro Rosenblatt, D.A.; Chan, D.S.; Vieira, A.R.; Vieira, R.; Greenwood, D.C.; Vatten, L.J.; Norat, T. Dairy products, calcium, and prostate cancer risk: A systematic review and meta-analysis of cohort studies. Am. J. Clin. Nutr. 2015, 101, 87–117. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Schwedhelm, C.; Kalle-Uhlmann, T.; Missbach, B.; Knuppel, S.; Boeing, H. Consumption of dairy products in relation to changes in anthropometric variables in adult populations: A systematic review and meta-analysis of cohort studies. PLoS ONE 2016, 11, e0157461. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Schwedhelm, C.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of type 2 diabetes mellitus: A systematic review and meta-analysis of prospective studies. Eur. J. Epidemiol. 2017, 32, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.G.; Sun, J.W.; Yang, Y.; Ma, X.; Wang, Y.Y.; Xiang, Y.B. Fish consumption and all-cause mortality: A meta-analysis of cohort studies. Eur. J. Clin. Nutr. 2016, 70, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Caygill, C.P.; Hill, M.J. Fish, n-3 fatty acids and human colorectal and breast cancer mortality. Eur. J. Cancer Prev. 1995, 4, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Szymanski, K.M.; Wheeler, D.C.; Mucci, L.A. Fish consumption and prostate cancer risk: A review and meta-analysis. Am. J. Clin. Nutr. 2010, 92, 1223–1233. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Lampousi, A.M.; Knuppel, S.; Iqbal, K.; Bechthold, A.; Schlesinger, S.; Boeing, H. Food groups and risk of all-cause mortality: A systematic review and meta-analysis of prospective studies. Am. J. Clin. Nutr. 2017, 105, 1462–1473. [Google Scholar] [CrossRef] [PubMed]
- Tavani, A.; Pelucchi, C.; Parpinel, M.; Negri, E.; Franceschi, S.; Levi, F.; La Vecchia, C. N-3 polyunsaturated fatty acid intake and cancer risk in Italy and Switzerland. Int. J. Cancer 2003, 105, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Chapkin, R.S.; Davidson, L.A.; Ly, L.; Weeks, B.R.; Lupton, J.R.; McMurray, D.N. Immunomodulatory effects of (n-3) fatty acids: Putative link to inflammation and colon cancer. J. Nutr. 2007, 137, 200s–204s. [Google Scholar] [PubMed]
- Schwingshackl, L.; Hoffmann, G.; Missbach, B.; Stelmach-Mardas, M.; Boeing, H. An umbrella review of nuts intake and risk of cardiovascular disease. Curr. Pharm. Des. 2017, 23, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Nut consumption and risk of cardiovascular disease, total cancer, all-cause and cause-specific mortality: A systematic review and dose-response meta-analysis of prospective studies. BMC Med. 2016, 14, 207. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Sun, Q.; Bernstein, A.M.; Schulze, M.B.; Manson, J.E.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Red meat consumption and mortality: Results from 2 prospective cohort studies. Arch. Intern. Med. 2012, 172, 555–563. [Google Scholar] [PubMed]
- Rohrmann, S.; Overvad, K.; Bueno-de-Mesquita, H.B.; Jakobsen, M.U.; Egeberg, R.; Tjønneland, A.; Nailler, L.; Boutron-Ruault, M.C.; Clavel-Chapelon, F.; Krogh, V.; et al. Meat consumption and mortality-results from the European Prospective Investigation into Cancer and Nutrition. BMC Med. 2013, 11, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Alcohol Consumption and Ethyl Carbamate; International Agency for Research on Cancer: Lyon, France, 2010; p. 1440. [Google Scholar]
- Allen, N.E.; Beral, V.; Casabonne, D.; Kan, S.W.; Reeves, G.K.; Brown, A.; Green, J.; Collaborators, M.W.S. Moderate alcohol intake and cancer incidence in women. J. Natl. Cancer Inst. 2009, 101, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Lachenmeier, D.W.; Rehm, J. Moderate red wine drinking does not help cut women’s breast cancer risk. J. Womens Health. (Larchmt) 2012, 21, 469–470. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Hunter, D.J.; Spiegelman, D.; Adami, H.O.; Albanes, D.; Bernstein, L.; van den Brandt, P.A.; Buring, J.E.; Cho, E.; Folsom, A.R.; et al. Alcohol intake and renal cell cancer in a pooled analysis of 12 prospective studies. J. Natl. Cancer Inst. 2007, 99, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Mack, W.J.; Preston-Martin, S.; Dal Maso, L.; Galanti, R.; Xiang, M.; Franceschi, S.; Hallquist, A.; Jin, F.; Kolonel, L.; La Vecchia, C.; et al. A pooled analysis of case-control studies of thyroid cancer: Cigarette smoking and consumption of alcohol, coffee, and tea. Cancer Causes Control 2003, 14, 773–785. [Google Scholar] [CrossRef] [PubMed]
- Morton, L.M.; Zheng, T.; Holford, T.R.; Holly, E.A.; Chiu, B.C.; Costantini, A.S.; Stagnaro, E.; Willett, E.V.; Dal Maso, L.; Serraino, D.; et al. Alcohol consumption and risk of non-Hodgkin lymphoma: A pooled analysis. Lancet Oncol. 2005, 6, 469–476. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The mediterranean diets: What is so special about the diet of Greece? The scientific evidence. J. Nutr. 2001, 131, 3065S–3073S. [Google Scholar] [PubMed]
- Trichopoulou, A.; Orfanos, P.; Norat, T.; Bueno-de-Mesquita, B.; Ocké, M.C.; Peeters, P.H.; van der Schouw, Y.T.; Boeing, H.; Hoffmann, K.; Boffetta, P.; et al. Modified Mediterranean diet and survival: EPIC-Elderly Prospective Cohort Study. BMJ 2005, 330, 991. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, A.; De Pergola, G. Mediterranean diet and cardiovascular disease: A critical evaluation of a priori dietary indexes. Nutrients 2015, 7, 7863–7888. [Google Scholar] [CrossRef] [PubMed]
- Verberne, L.; Bach-Faig, A.; Buckland, G.; Serra-Majem, L. Association between the Mediterranean diet and cancer risk: A review of observational studies. Nutr. Cancer 2010, 62, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Lampousi, A.M.; Portillo, M.P.; Romaguera, D.; Hoffmann, G.; Boeing, H. Olive oil in the prevention and management of type 2 diabetes mellitus: A systematic review and meta-analysis of cohort studies and intervention trials. Nutr. Diabetes 2017, 7, e262. [Google Scholar] [CrossRef] [PubMed]
- Cicerale, S.; Conlan, X.A.; Sinclair, A.J.; Keast, R.S. Chemistry and health of olive oil phenolics. Crit. Rev. Food Sci. Nutr. 2009, 49, 218–236. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.; Forman, D.; Bray, F. Globocan 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC Cancerbase No. 11. Available online: http://www.wcrf.org/int/cancer-facts-figures/data-cancer-frequency-country (accessed on 25 July 2017).
- Imamura, F.; Micha, R.; Khatibzadeh, S.; Fahimi, S.; Shi, P.; Powles, J.; Mozaffarian, D.; Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (NutriCoDE). Dietary quality among men and women in 187 countries in 1990 and 2010: A systematic assessment. Lancet Glob. Health 2015, 3, e132–e142. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Hoffmann, G. Diet quality as assessed by the Healthy Eating Index, the Alternate Healthy Eating Index, the Dietary Approaches to Stop Hypertension score, and health outcomes: A systematic review and meta-analysis of cohort studies. J. Acad. Nutr. Diet. 2015, 115, 780–800. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Autier, P. Prevalence of main cancer lifestyle risk factors in europe in 2000. Eur. J. Cancer 2010, 46, 2534–2544. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Pooled risk ratios of individual Mediterranean diet components and overall cancer risk.


{kind=link}
Table 1.
General study characteristics of included studies (randomized controlled trials, cohort and case-control studies).
Table 1.
General study characteristics of included studies (randomized controlled trials, cohort and case-control studies).
| Author | Country Study Name | Study Design | Outcome | Population Follow-Up (Years) | Age at Entry | Sex | Components of Score Score Range | Adjustment | RR/HR/OR (95% CI) Multivariable Adjusted |
|---|---|---|---|---|---|---|---|---|---|
| De Lorgeril et al. [32] | France Lyon Diet Heart Study | RCT | Cancer mortality Lung cancer Digestive tract cancer Urinary tract cancer Throat cancer | 605 4 | 54 | M/W | 1. MedD: More bread, more root vegetables and green vegetables, more fish, less meat, no day without fruit, and butter and cream to be replaced with margarine supplied by the study; supplemented with a rapeseed oil-based margarine 2. control diet | NA | Cancer mortality MedD with margarine RR: 0.75 (0.17, 3.33) versus control diet Lung cancer MedD with margarine RR: 2.01 (0.37, 10.87) versus control diet Throat cancer MedD with margarine RR: 0.14 (0.01, 2.76) versus control diet |
| Toledo et al. [33] | Spain PREDIMED | RCT | Breast cancer | 4282 4.8 | 60–80 | W | 1. MedD supplemented with extra-virgin olive oil; 2. MedD supplemented with mixed nuts; 3. control diet (advice to reduce dietary fat) | Age, study site, BMI, waist-to-height ratio, hormone therapy, PA, total energy intake, alcohol, age at menopause, baseline adherence to the MedD | MedD with olive oil RR: 0.32 (0.13, 0.79) versus control diet MedD with nuts RR: 0.59 (0.26, 1.35) versus control diet Both MedD RR: 0.43 (0.21, 0.88) versus control diet |
| Anic et al. [50] | United States NIH-AARP | Cohort | Lung cancer | 460,770 10.5 | 50–71 | M/W | 1.↑ whole grains; 2.↑ vegetables; 3.↑ fruits; 4.↑ nuts; 5.↑ legumes; 6.↑ fish; 7.↑ MUFA:SFA ratio; 8.↓ red and processed meats; 9.↔ alcohol MedD score range: 0–9 | Age, sex, race, education, BMI, PA, total energy, smoking status, cigarettes per day, time since quitting smoking, and regular use of cigars/pipes | HR: 0.85 (0.79, 0.91) for fifth versus first quintile |
| Butler et al. [64] | Singapore SCHS | Cohort | Breast cancer | 34,028 >5 | 45–74 | W | 1.↑ cereals; 2.↑ vegetables; 3.↑ fruits/nuts; 4.↑ legumes; 5.↑ fish; 6.↑ MUFA: SFA ratio; 7.↓ meat; 8.↓ dairy; 9.↓ carbohydrates; 10. ↓ alcohol MedD score range: 0–10 | NA | HR: 0.96 (0.76, 1.21) for third versus first tertile |
| Dugué et al. [51] | Australia MCCS | Cohort | Urothelial cell carcinoma | 37,442 21.3 | 40–69 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ cereals; 4.↑ legumes; 5.↑ fish; 6.↑ olive oil; 7.↓ dairy; 8.↓ red meat; 9.↔ alcohol MedD score range: 0–9 | Sex, country of birth, smoking, alcohol, BMI, PA, education, socioeconomic status | HR: 0.89 (0.62, 1.26) for fifth versus first quintile |
| Haridass et al. [52] | United States CTS | Cohort | Breast cancer | 90,244 16 | 22–104 | W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts/legumes; 4.↑ fish; 5.↑ whole grains; 6.↑ MUFA:SFA; 7.↓ red and processed meats; 8.↔ alcohol MedD score range: 0–8 | Age at baseline, race, menopausal status, age at menarche, breast cancer family history, smoking, BMI, energy intake | HR: 0.91 (0.83, 1.01) for fifth versus first quintile |
| Hirko et al. [53] | United States NHS | Cohort | Breast cancer (by molecular subtype) | 100,643 22 | 30–55 | W | 1.↑ fruits; 2.↑ vegetables; 3.↑ legumes and soy; 4.↑ nuts; 5.↑ fish and seafood; 6.↑ whole grains; 7.↑ MUFA:SFA; 8.↓ red and processed meat; 9.↔ alcohol MedD score range: 0–9 | BMI at age 18, weight change since age 18, PA, energy intake, parity/age at first birth, menopausal hormone use, oral contraceptive use, age at menarche, age at menopause, family history of breast cancer, benign breast cancer diagnosis | Luminal A HR: 1.09 (0.91, 1.30) for fifth quintile (5.5–9.0) versus first (0–2.6) quintile Luminal B HR: 1.02 (0.76, 1.37) for fifth quintile (5.5–9.0) versus first (0–2.6) quintile HER2 type HR: 0.74 (0.42, 1.29) for fifth quintile (5.5–9.0) versus first (0–2.6) quintile Basal-like HR: 0.78 (0.49, 1.26) for fifth quintile (5.5–9.0) versus first (0–2.6) quintile Unclassified HR: 0.89 (0.41, 1.89) for fifth quintile (5.5–9.0) versus first (0–2.6) quintile |
| Hodge et al. [54] | Australia MCCS | Cohort | Lung cancer | 35,303 18 | 40–69 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ cereals; 4.↑ legumes; 5.↑ fish; 6.↑ olive oil; 7.↓ dairy; 8.↓ red meat; 9.↔ alcohol MedD score range: 0–9 | Pack-years, years since quitting smoking, smoking status, country of birth, education, BMI, PA, sex, SEIFA quintile, energy | HR: 0.64 (0.45, 0.90) for highest category (7–9) versus lowest category (0–3) |
| Jacobs et al. [55] | United States MEC | Cohort | Colorectal cancer mortality among cancer survivors | 4204 6.0 | 45–75 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts; 4.↑ legumes; 5.↑ fish; 6.↑ whole grains; 7.↑ MUFA:SFA; 8.↓ red and processed meat; 9.↔ alcohol MedD score range: 0–9 | Age at diagnosis, ethnicity, stage at diagnosis, total energy intake, smoking status, pack-years, PA, education, radiation treatment, chemotherapy, NSAID use, family history of CRC, comorbidities | Men HR: 1.07 (0.81, 1.42) for fourth quartile (6–9) versus first quartile (0–2) Women HR: 0.74 (0.54, 1.01) for fourth quartile (6–9) versus first quartile (0–2) |
| Jones et al. [65] | United Kingdom WHS | Cohort | Colorectal cancer | 35,372 17.4 | 35–69 | W | 1.↑ vegetables; 2.↑ fruits & nuts; 3.↑ legumes; 4.↑ cereals; 5.↑ fish; 6.↑ MUFA+PUFA: SFA; 7.↓ dairy; 8.↓ meat; 9. ↓ poultry; 10.↔ alcohol MedD score range: 0–10 | Age, BMI, energy intake, physical activity, smoking status, socioeconomic status and family history of colorectal cancer | HR: 0.82 (0.57, 1.17) Fifth quintile (7–10) versus first quintile (0–2) |
| Larsson et al. [56] | Sweden Swedish Mammography Cohort Cohort of Swedish Men | Cohort | Biliary tract cancer Gallbladder cancer | 76,014 13.3 | 45–83 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ legumes and nuts; 4.↑ whole-grains; 5.↑ fish; 6.↓ full-fat dairy products; 7.↓ red meat and processed meat; 8.↑ olive oil; 9.↔ alcohol MedD score range: 9–45 | Age, sex, education, smoking status and pack-years of smoking, diabetes, BMI, total energy intake | Extrahepatic Biliary tract cancer HR: 0.41 (0.25, 0.67) for third tertile (29–45) to first tertile (9–24) Gallbladder cancer HR: 0.42 (0.23, 0.79) for third tertile (29–45) to first tertile (9–24) Intrahepatic BTC HR: 0.71 (0.25, 2.04) for third tertile (29–45) to first tertile (9–24) |
| Lassale et al. [57] | Europe EPIC | Cohort | Cancer mortality | 451,256 12.8 | 25–70 | M/W | MedD: 1. fruits; 2. vegetables; 3. legumes; 4. grains; 5. fish; 6. meat; 7. dairy products; 8. MUFA:SFA; 9. alcohol MedD score range: 0–9 rMedD: 1. fruits; 2. vegetables; 3. legumes; 4. grains; 5. fish; 6. meat; 7. dairy products; 8. olive oil; 9. alcohol rMED score range: 0–18 MSDPS: 1. whole grain cereals (8 servings/day); 2. fruits (3 servings/day); 3. vegetables (6 servings/day); 4. dairy (2 servings/day); 5. fish (6 servings/week); 6. wine (3 and 1.5 servings/day for men and women, respectively); 7. poultry (4 servings/week); 8. olives, legumes, and nuts (4 servings/week); 9. potatoes (3 servings/week); 10. eggs (3 servings/week); 11. sweets (3 servings/week); 12. meats (1 servings/week); 13. olive oil (exclusive use) MSDPS score range: 0–100 | Age at baseline, BMI, PA, smoking status, education, stratified by sex and study center | MedD HR: 0.82 (0.77, 0.88) for fourth versus first quartile rMED HR: 0.82 (0.77, 0.88) for fourth versus first quartile MSDPS HR: 0.84 (0.79, 0.90) for fourth versus first quartile |
| Maisonneuve et al. [58] | Italy COSMOS | Cohort | Lung cancer | 4336 8.5 | 50–84 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts; 4.↑ cereals; 5.↑ legumes; 6.↑ fish; 7.↓ red and processed meats; 8.↔ alcohol; 9.↑ MUFA:SFA MedD score range: 0–9 | Baseline risk probability (age, sex, smoking duration, smoking intensity, years of smoking cessation, asbestos exposure), total energy, dietary inflammatory index | HR: 0.20 (0.04, 0.91) for highest score category (8–9) versus lowest score category (0–1) |
| Molina-Montes et al. [59] | Europe EPIC | Cohort | Exocrine pancreatic cancer | 477,309 11.3 | 35–70 | M/W | 1.↑ fruits and nuts; 2.↑ vegetables; 3.↑ legumes; 4.↑ fish and seafood; 5.↑ olive oil; 6.↑ cereals; 7.↓ meat; 8.↓ dairy products MedD score range: 0–16 | Total energy intake, BMI, smoking status and intensity, alcohol intake, diabetes, stratified by age, sex and study centre | HR: 0.99 (0.77, 1.26) for highest score category (10–16) versus lowest score category (0–5) |
| Park et al. [60] | United States MEC | Cohort | Colorectal cancer | 190,949 16 | 45–75 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts; 4.↑ legumes; 5.↑ fish; 6.↑ whole grains; 7.↑ MUFA:SFA; 8.↓ red and processed meat; 9.↔ alcohol MedD score range: 0–9 | Age at cohort entry, family history of colorectal cancer, history of colorectal polyp, BMI, smoking, multivitamin, nonsteroidal anti-inflammatory drugs, physical activity, menopausal status, menopausal hormone therapy use for women only, and total energy intake | HR: ♂ 0.84 (0.72, 0.97) HR: ♀ 0.96 (0.82, 1.13) for highest score category (6–9) versus lowest score category (0–2) |
| Van den Brandt et al. [61] | The Netherlands NCS | Cohort | Breast cancer | 62,573 | 55–69 | W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts; 4.↑ whole grains; 5.↑ legumes; 6.↑ fish; 7.↑ MUFA:SFA; 8.↓ red and processed meats; 9.↔ alcohol MedD score range: 0–9 | Age, smoking, duration, body height, BMI, non-occupational physical activity, highest level of education, family history of breast cancer in mother or sisters, history of benign breast disease, age at menarche, parity, age at first birth, age at menopause, oral contraceptive use, postmenopausal HRT, energy intake and alcohol intake | HR: 0.87 (0.72, 1.06) for highest score category (6–8) vs. lowest score category (0–3) Without alcohol component |
| Vargas et al. [62] | United States WHIOS | Cohort | Colorectal cancer | 78,273 12.4 | 50–79 | W | 1.↑ vegetables; 2.↑ fruits; 3.↑ nuts; 4.↑ whole grains; 5.↑ legumes; 6.↑ fish; 7.↑ MUFA:SFA; 8.↓ red and processed meats; 9.↔ alcohol MedD score range: 0–9 | Age, race/ethnicity, PA, education, smoking, hormone replacement therapy | HR: 0.91 (0.74, 1.11) for fifth quintile (6–9) versus first quintile (0–2) |
| Whalen et al. [63] | United States REGARDS | Cohort | Cancer mortality | 21,423 6.25 | >45 | M/W | 1.↑ vegetables; 2.↑ fruits; 3.↑ lean meats; 4.↑ fish; 5.↑ nuts; 6.↑ MUFA:SFA; 7.↓ red and processed meats; 8.↓ sodium; 9. ↔ dairy; 10.↔ grains and starches; 11.↔ alcohol MedD score range: 11–55 | Sex, race, total energy intake, BMI, PA, smoking, annual income, hormone replacement therapy use (in women) at baseline | HR: 0.64 (0.48, 0.84) for fifth versus first quintile |
| Author | Country Study Name | Study Design | Outcome | Cases/Controls | Age at Entry | Sex | Components of Score Score Range | Adjustment | Multivariable Adjusted |
| Askari et al. [66] | Iran | Case-control | Prostate cancer | 52/104 | 40–78 | M | 1. whole grain cereals (8 servings/day); 2. fruits (3 servings/day); 3. vegetables (6 servings/day); 4. dairy products (2 servings/day); 5. fish and other seafood (6 servings/week); 6. poultry (4 servings/week); 7. olives/legumes/nuts (4 servings/week); 8. potatoes and other starchy roots (3 servings/week); 9. eggs (3 servings/week); 10. sweets (3 servings/week); 11. meat (1 servings/week); 12. olive oil (exclusive use) MedD score range: 0–100 | Age, BMI, smoking, energy intake, education, diabetes | OR: 0.28 (0.08, 0.91) for third versus first tertile |
| Campagna et al. [67] | Italy | Case-control | Lymphoma | 322/446 | n.d | M/W | 1.↑ fruits; 2.↑ vegetables; 3.↑ legumes; 4.↑ fresh fish and seafood; 5.↑ pasta, rice, and bread; 6.↓ red meat; 7.↔ wine MedD score range: n.d | Age, sex, education | OR: 0.9 (0.6, 1.5) for fifth versus first quintile |
| Castello et al. [43] | Spain | Case-control | Breast cancer | 1181/1682 | 20–85 | W | PCA: ↑ fish; ↑ vegetables; ↑ legumes; ↑ boiled potatoes; ↑ fruits; ↑ olives and vegetable oil; ↓ juices | menopausal status, age, education, BMI, age at first delivery, family history of breast cancer, physical activity, smoking status, caloric intake and alcohol intake as fixed effects and province of residence as a random effect term | OR: 0.90 (0.69, 1.17) for fourth vs. first quartile |
| Castello et al. [44] | Spain | Case-control | Prostate cancer | 754/1277 | 38–85 | M | PCA: ↑ fish; ↑ vegetables; ↑ legumes; ↑ boiled potatoes; ↑ fruits; ↑ olives and vegetable oil; ↓ juices | Age, education, BMI, age at first delivery, family history of prostate cancer and caloric intake as fixed effects and province of residence as a random effect | OR: 0.91 (0.66, 1.25) for fourth vs. first quartile |
| Giraldi et al. [68] | Italy | Case-control | Head and neck cancer | 500/433 | n.d | M/W | 1.↑ fruits; 2.↑ vegetables; 3.↑ legumes; 4.↑ fish; 5.↓ meat and meat products; 6.↔ alcohol MedD score range: 0–12 | Age, sex, smoking, alcohol, total energy intake | OR: 0.64 (0.58, 0.71) per 1-point increase |
| Rosato et al. [69] | Italy | Case-control | Colorectal cancer | 3745/6804 | 19–74 | M/W | 1.↑ vegetables; 2.↑ legumes; 3.↑ fruits and nuts; 4.↑ cereals; 5.↑ fish and seafood; 6.↑ MUFA:SFA; 7.↓ dairy; 8.↓ meat and meat products; 9.↔ alcohol MedD score range: 0–9 | Age, sex, calendar period, center, education, BMI, PA, family history of intestinal cancer, total energy intake | OR: 0.52 (0.43, 0.62) for highest score category (7–9) versus lowest score category (0–2) |
| Stojanovic 2017 [70] | Italy | Case-control | Gastric cancer | 223/223 | NA | NA | NA | NA | OR: 0.70 (0.61, 0.81) |
| Turati et al. [71] | Italy | Case-control | Nasopharyngeal cancer | 198/594 | 18–76 | M/W | 1.↑ vegetables; 2.↑ legumes; 3.↑ fruits and nuts; 4.↑ cereals; 5.↑ fish and seafood; 6.↑ MUFA:SFA; 7.↓ dairy products; 8.↓ meats; 9.↔ alcohol MedD score range: 0–9 | sex, age, place of residence, education, smoking, total energy intake | OR: 0.66 (0.44, 0.99) for highest score category (>6) versus lowest score category (0–4) |
| Wang et al. [72] | China | Case-control | Nasopharyngeal cancer | 600/600 | M/W | 1.↑ whole grains; 2.↑ vegetables; 3.↑ fruits; 4.↑ legumes; 5.↑ nuts; 6.↑ fish; 7.↑ MUFA:SFA; 8.↔ alcohol; 9.↓ red and processed meats MedD score range: 0–9 | Age, BMI, occupation, marital status, education, household income, smoking, drinking, exposure to potential toxic substances, multivitamin supplements, chronic rhinitis history, PA, energy intake, preserved vegetables and animal food | OR: 0.85 (0.59, 1.22) for fourth versus first quartile |
BMI, Body Mass Index; HR, Hazard ratio; M, men; MedD, Mediterranean Diet; MSDPS, Mediterranean Style Dietary Pattern Score; MUFA, monounsaturated fat; NA, not applicable; OR, Odds ratio; PA, physical activity; PCA, principal component analysis; PUFA, polyunsaturated fat; RCT, randomized controlled trials; rMedD, relative Mediterranean diet score; RR, Risk ratio; SFA, saturated fatty acids; W, women.
Table 2.
Risk ratio/odds ratio associated with the highest adherence to Mediterranean dietary pattern.
Table 2.
Risk ratio/odds ratio associated with the highest adherence to Mediterranean dietary pattern.
| Outcome | No. of Studies | Study Type | Risk Ratio/Odds Ratio | 95% CI | I2 (%) |
|---|---|---|---|---|---|
| Cancer mortality | 1 | RCT | 0.75 | 0.17, 3.33 | NA |
| 14 | Cohort | 0.86 | 0.81, 0.91 | 82 | |
| Colorectal cancer | 11 | Observational | 0.82 | 0.75, 0.88 | 73 |
| incidence | 6 | Cohort | 0.86 | 0.80, 0.92 | 28 |
| 5 | Case-control | 0.71 | 0.57, 0.88 | 88 | |
| Breast cancer | 1 | RCT | 0.43 | 0.21, 0.88 | NA |
| 16 | Observational | 0.92 | 0.89, 0.96 | 8 | |
| incidence | 7 | Cohort | 0.94 | 0.90, 0.99 | 11 |
| 9 | Case-control | 0.89 | 0.85, 0.94 | 0 | |
| Prostate cancer | 6 | Combined | 0.96 | 0.92, 1.00 | 0 |
| incidence | 3 | Cohort | 0.96 | 0.92, 1.00 | 0 |
| 3 | Case-control | 0.90 | 0.64, 1.26 | 52 | |
| Gastric cancer | 4 | Combined | 0.72 | 0.60, 0.86 | 55 |
| incidence | 2 | Cohort | 0.82 | 0.61, 1.10 | 49 |
| 2 | Case-control | 0.65 | 0.53, 0.79 | 53 | |
| Liver cancer | 2 | Combined | 0.58 | 0.46, 0.73 | 0 |
| incidence | 1 | Cohort | 0.62 | 0.47, 0.82 | NA |
| 1 | Case-control | 0.51 | 0.34, 0.77 | NA | |
| Esophageal cancer | 2 | Combined | 0.49 | 0.22, 1.09 | 83 |
| incidence | 1 | Cohort | 0.68 | 0.34, 1.36 | NA |
| 1 | Case-control | 0.26 | 0.13, 0.52 | NA | |
| Head and neck cancer | 1 | RCT | 0.14 | 0.01, 2.76 | 86 |
| 7 | Observational | 0.49 | 0.37, 0.66 | 87 | |
| incidence | 1 | Cohort | 0.61 | 0.33, 1.14 | 77 |
| 6 | Case-control | 0.46 | 0.32, 0.67 | 89 | |
| Endometrial cancer | 3 | Combined | 0.72 | 0.40, 1.31 | 94 |
| incidence | 1 | Cohort | 0.98 | 0.82, 1.17 | NA |
| 2 | Case-control | 0.61 | 0.29, 1.29 | 89 | |
| Respiratory cancer | 1 | RCT | 2.01 | 0.37, 10.87 | NA |
| incidence | 3 | Cohort | 0.71 | 0.49, 1.02 | 66 |
| Bladder cancer incidence | 2 | Cohort | 0.85 | 0.72, 1.01 | NA |
| Pancreatic cancer | 2 | Combined | 0.69 | 0.34, 1.41 | 92 |
| 1 | Cohort | 0.99 | 0.77, 1.27 | NA | |
| 1 | Case-control | 0.48 | 0.35, 0.66 | NA | |
| Gallbladder cancer | 1 | Cohort | 0.42 | 0.23, 0.77 | NA |
| Biliary tract cancer | 1 | Cohort | 0.44 | 0.29, 0.67 | NA |
| Ovarian cancer | 1 | Cohort | 0.91 | 0.71, 1.17 | NA |
| Lymphoma | 1 | Case-control | 0.90 | 0.60, 1.35 | NA |
| Cancer mortality among cancer survivors | 4 | Cohort | 0.95 | 0.82, 1.12 | 5 |
| Recurrence among cancer survivors | 1 | Cohort | 0.61 | 0.18, 2.07 | NA |
CI, confidence interval; NA, not applicable; RCT, randomized controlled trial.
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients 2017, 9, 1063. https://doi.org/10.3390/nu9101063
AMA Style
Schwingshackl L, Schwedhelm C, Galbete C, Hoffmann G. Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis. Nutrients. 2017; 9(10):1063. https://doi.org/10.3390/nu9101063
Chicago/Turabian StyleSchwingshackl, Lukas, Carolina Schwedhelm, Cecilia Galbete, and Georg Hoffmann. 2017. "Adherence to Mediterranean Diet and Risk of Cancer: An Updated Systematic Review and Meta-Analysis" Nutrients 9, no. 10: 1063. https://doi.org/10.3390/nu9101063
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.